
تضخم الطحال /من ويكيبيديا،
الموسوعة الحرة
الطَّحَل

تصوير مقطعي محوسب يظهر فيه طَحَل لدى مريض يعاني من
ابيضاض لمفاوي مزمن
معلومات عامة
الاختصاص جراحة عامة
الطَّحَلُ أو تَضَخُّمُ الطَّحَالِ
(بالإنجليزية:
Splenomegaly)
هو ازدياد حجم الطحال. يقع الطحال في الربع العلوي الأيسر من بطن الإنسان. يعتبر
تضخم الطحل واحد من أربعة العلامات الأساسية لفرط نشاط الطحال، انخفاض معين في عدد
خلايا الدم الجائلة مؤديًا إلى أي مزيج من انخفاض كمية الخلايا المُحبّبة، خلايا
الدم الحمراء أو الصفائح الدموية;
استجابة تكاثرية تعويضية في نقي العظم; وقابلية تصحيح
هذه العيوب عن طريق استئصال الطحال.
تعريف
لا يجب الخلط بين تضخم الطحال وتوحش الطحال، فتضخم
الطحال يعني زيادة حجم الطحال مع أو بدون اضطراب وظائفه. أما توحش الطحال فيعني
اضطراب وظائف الطحال حيث يقوم بتكسير خلايا الدم البيضاء وكرات الدم الحمراء
والصفائح قبل اكتمال عمرها الافتراضي وقد يحدث ذلك بوجود زيادة في حجم الطحال أو
بدون. وقد يصاب المريض بأحد الأثنين أو كلاهما معًا في وقت واحد.
صنّف الطبيب باولين وفريق عمله في ورقة بحثية منشورة
تضخم الطحال على النحو التالي: طحل معتدل إذا كان البعد
الأكبر للطحال يتراوح بين الـ 11-20 سم
طحل شديد إذا كان البعد الأكبر للطحال أكبر من 20 سم
وكلينيكيًا ففي الحالة الطبيعية يكون الطحال عضو غير
محسوس بواسطة الفحص اليدوي للطبيب، وإن استطاع الطبيب أن يحسّ ولو جزء من الطحال
بالفحص عندها يتم اعتبار الطحال متضخمًا، وذلك في البالغين. أما في حديثي الولادة
فإن الطبيب يمكنه بالفحص اليدوي إحساس الطحال وحتى عمر 3 شهور.
الأعراض
قد تشمل أعراض الطَحَل ألم بطني، ألم الصدر، وألم صدر
شبيه بألم الصدر الجنبي عند امتلاء المعدة، المثانة البولية أو الأمعاء، وآلام
الظهر، والشبع المبكّر بسبب تضخم الطحال، أو أعراض أخرى لفقر الدم بسبب قلة
الكريات.
العلامات
بالفحص السريري يمكن للطبيب أن يحس بيده الحافة السفلية
للطحال تحت حافة الضلوع اليسرى، كما يمكنه سماع صوت مميز للطحال المتضخم بواسطة
السماعة الطبية. ولابد من تأكيد التشخيص بواسطة التصوير التليفزيوني على البطن
أو أشعة الرنين المغناطيسي.
أسبابالأسباب الأكثر شيوعًا للتضخم الطحال في البلدان
المتقدمة هي مرض كثرة الوحيدات العدوائية، واختراق الطحال من قبل خلايا سرطانية من
ورم دموي خبيث، وفرط ضغط الدم البابي (في معظم الحالات ثانوي لمرض الكبد،
وساركويد). وقد ينبع كذلك الطحل من الالتهابات الجرثومية، مثل الزهري أو عدوى تصيب
الطبقة الداخلية في لقلب (إلتهاب الشغاف).
تشمل الأسباب المحتملة للطَحل الشديد (الطحال العملاق)
وفيه يكون وزن الطحال > 1000
غرام: الإصابة بالبلهارسيا
الملاريا
داء الليشمانيات الحشوي
ابيضاض الدم النقوي المزمن
تليف نقوي وهو سرطان نادر يصيب نخاع العظام
تشمل الأسباب المحتملة للطَحَل المعتدل وفيه يكون وزن
الطحال <1000 غرام :
أسباب تضخم الطحال مصنفة إلى مجموعات حسب السبب إزدياد
الوظيفة تدفق دم غير طبيعي إرتشاح
وظيفة تكسير كريات الدم الحمراء التالفة كثرة الكريات
الحمر الكروية
ثلاسيميا
إعتلال هيموغلوبيني
فقر الدم المتعلق بالغذاء
فقر الدم المنجلي المبكر
الوظيفة المناعية
العدوى البكتيرية والفيروسية والطفيلية كثرة الوحيدات
العدوائية، الإيدز,
التهاب الكبد الفيروسي
التهاب الشغاف البكتيري الحاد، تسمم الدم
خرّاج الطحال, حمى التيفويد
داء البروسيلات، داء البريميات، السل الرئوي
داء النوسجات
ملاريا، داء الليشمانيات، داء المثقبيات
أمراض اضطراب المناعة التهاب المفاصل الروماتويدي
ذئبة حمامية شاملة
داء المصل
داء البلعمة
فقر الدم الانحلالي بالمناعة الذاتية
مرض التكاثر الليمفاوي وهي مجموعة من الأمراض التي يتم
فيها زيادة الخلايا الليمفاوية بشكل غير طبيعي وغير منتظم
ساركويد
التفاعلات الدوائية
وظيفة تكوين الدم خارج النقي(الجزء من العظام المسؤول عن
تصنيع الدم) وفيه يفضل نخاع العظام في القيام بوظيفته في تكوين خلايا الدم فتنتقل
هذه الوظيفة إلى أعضاء أخرى هي الكبد والطحال مما يسبب زيادة حجمهما تليّف نقوي
وهو ورم سرطاني يصيب نخاع العظم مما يؤدي إلى تحول عملية تصنيع الدم إلى الكبد والطحال
أورام الدم ونخاع العظم لوكيميا
تعرض نخاع العظم للإشعاع مما يسبب فشله وتوقف وظيفته فشل
عضوي تشمع الكبد مما يسبب احتقان الدم داخل الطحال وتضخمه
وعائي إنسداد الوريد الكبديّ
إنسداد الوريد البابيّ (متلازمة بانتي) : وهو المسؤول عن
نقل الدم من الطحال والجهاز الهضمي إلى الكبد
متلازمة بود كياري
إنسداد الوريد الطحاليّ : وهو المسؤول عن نقل الدم من
الطحال إلى الالوريد الأجوف السفلي ومنه إلى القلب
حالات عدوى داء البلهارسيات الكبدي
داء المشوكات أمراض استقلابية داء غوشيه
داء نيمان بيك
داء الألفا مانوزيدي
متلازمة هيرلر وداء عديد السكاريد المخاطي
داء نشواني
عوز البروتين الشحمي العائلي
أورام حميدة أو خبيثة لوكيميا بأنواعها
ليمفوما بأنواعها
مرض تكاثر نقوي
هجرة خلايا سرطانية من أي عضو إلى الطحال
داء كثرة المنسجات X
ورم وعائي دموي، ورم لمفي
تكيسات الطحال
ورم عابي
ورم حبيبي حلقي
العلاج
إن كانت حالة تضخم الطحال مصاحبة لحالة توحش الطحال
فلابد من إجراء جراحة استئصال الطحال, مع استمرار إجراء الفحوص واتخاذ العلاجات
اللازمة لعلاج السبب إن أمكن.
ولأن الطحال دور هام في المناعة والدفاع عن الجسم ضد البكتيريا
والفيروسات فإنه في حالة تقرير استئصال الطحال كعلاج لمريض ما لابد من تطعيم هذا
المريض قبل العملية بعدة تطعيمات ضد بكتيريا المستدمية النزلية التي تتسبب في
التهاب رئوي والتهاب سحائي مميت، وضد بكتيريا المكورة الرئوية وبكتيريا المكورة
السحائية. ولابد أن يتعاطى المريض أيضًا التطعيم ضد الإنفلونزا سنويًا، وفي بعض
الحالات قد يوصف للمريض مضادات حيوية للوقاية.
انظر أيضًانقص الجالاكتوز إبيميراس
متلازمة أومين
علامة سريرية
متلازمة بانتي
فرط ضغط الدم البابي
انعدام الطحال
ضخامة الأعضاء
======
نقص الجالاكتوز إبيميراس
من ويكيبيديا، الموسوعة الحرة
نقص إيبيميراز الجالاكتوز
معلومات عامة
من أنواع وجود الغالاكتوز في الدم، واضطراب صبغي جسدي
متنحي

نقص الجالاكتوز إبيميراس، المعروف أيضا باسم نقص غيل،
غالاكتوسيميا الثالث ونقص أودب الجالاكتوز -4 إبيميراس،
هو نادر، شكل متنحية مقهورة من الجالاكتوز في الدم يرتبط
مع نقص في إبيميراس انزيم غالاكتوز.
الأعراض أعراض الجلوكتوزيميا النوع الثالث هي واضحة من
الولادة، ولكن تختلف في شدة اعتمادا على ما إذا كان شكل المرض المحيطي أو المعمم
موجود. قد تشمل الأعراض:
اليرقان عند الأطفال
نقص التوتر الطفولي
ملامح ديسمورفيك
فقدان السمع الحسي العصبي
إعاقة النمو
أوجه القصور الإدراكي
استنفاد خلايا بوركينجي المخيخ
فشل المبيض (بوي) و هيبيرغوناديسم الضخامي
تليف كبدى
الفشل الكلوي
تضخم الطحال إعتام عدسة العين
دراسات النوع الثالث لأعراض الجالاكتوز في الدم هي في
معظمها وصفية، وتبقى الآليات المسببة للأمراض الدقيقة غير معروفة. ويرجع ذلك إلى
حد كبير إلى عدم وجود نماذج حيوانية وظيفية من الجالاكتوز في الدم الكلاسيكية.
التطور الأخير من ذبابة الفاكهة ميلانوغاستر غيل متحولة المعرض أعراض الجالكتوزيميا
قد تسفر عن نموذج الحيوان في المستقبل واعدة.
علم الوراثة
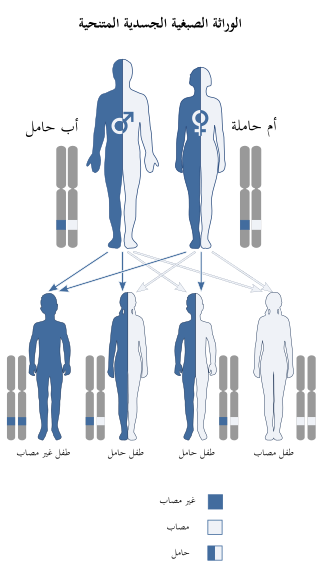
نقص الجالاكتوز إبيميراس لديه نمط وراثي متنحي.
الجالاكتوز إبيميراس نقص هو اضطراب متنحي وراثي،
وهو ما يعني أن الجين المعيب يقع على جسيم أوتوسوم،
ونسختين من الجين المعيب - واحد من كل الوالدين - مطلوبة لترث هذا الاضطراب. يحمل والدا
الفرد المصاب باضطراب جسمي متنحي نسخة واحدة من الجين المعيب، ولكن عادة لا يعاني
من أي علامات أو أعراض للاضطراب.
أساس وراثيوقد تم تحديد الطفرات غيل البشرية المختلفة
مما أدى إلى نوع 3 الجالاكتوز في الدم.
تحليل وظيفي من هذه الأشكال الإسعافية غيل متحولة تشير
إلى أن انخفاض الكفاءة التحفيزية وزيادة احتمال هضم بروتين تعمل بشكل سلبي في
النوع الثالث من الجالاكتوز في الدم.
بقايا متحوله تأثير البيوكيميائية المظاهر السريرية
V94M, K257R, L313M, R335H ضعف شديد وعدد دوران وخصوصية
ثابتة شديد الجالاكتوز في الدم المعمم.
S81R, T150M, P293L انخفاض عدد دوران معتدل الجالاكتوز
في الدم وسيطة.
L183P, D103G, G90E, N34S ضعف شديد ورقم دوران وخصوصية
ثابتة. وزيادة الهضم بروتين. الجالاكتوز في الدم معمم شديد.
أساس الكيمياء الحيوية
مسارات، وسيطة، والانزيمات المشاركة في استقلاب
الجالاكتوز.
نقص غيل يحول دون تجديد أودب الجلوكوز، ومنع تشكيل
الجلوكوز -1 الفوسفات ويؤدي إلى تراكم الجلاكتوز والجلاكتوز -1 الفوسفات. وقد تبين
أن مستويات عالية من الجالاكتوز -1 الفوسفات تتداخل مع فوسفهوغلوكوموتاز،
فوسفوريلاز الجليكوجين، أودب-غليكوبيروفوسفوريلاز، ونشاط مونوفوسفهاتاز إينوزيتول
في النماذج البكتيرية وفي المختبر، ولكن في الجسم الحي سمات آليات لم يتم تأكيدها
بعد. بغض النظر عن، متوسط مستويات الجالاكتوز -1 الفوسفات بمثابة التنبؤات الأكثر
دقة لشدة الأعراض المرتبطة النوع الثالث من الجالاكتوز في الدم.
انسداد مسار ليلور عن طريق نقص غيل أو اختلال وظيفي ينشط
مسارات بديلة من استقلاب الجلوكوز ويؤدي إلى تشكيل غالاكتيتول وغالاكتونات. يتم استقلاب
غالاكتونت بواسطة مسار الفوسفات البنتوز، ولا يعتبر سامة. غالاكتيتول، ومع ذلك، قد تتراكم في
ألياف العدسة، وتضارب عدسة نفاذية الخلايا الظهارية وتؤدي إلى موت الخلايا وتشكيل
الساد.
غيل نقص أيضا يتلوى جليكوليبيد والبروتين سكري بسبب
انخفاض إنتاج أودب-غالناك من أودب-غلناك.
التشخيصالفحص للكشف عن مستويات الجالاكتوز مرتفعة قد كشف
نقص غيل أو اختلال وظيفي لدى الرضع، ودراسات طفرة ل غيل متاحة سريريا.
تصنيف
هناك نوعان من نقص إبيميراس: نقص حميدة ونقص الكبد
الحاد. شكل حاد يشبه الجالاكتوز في الدم.
العلاجالأفراد الذين يعرضون مع النوع الثالث من
الجالاكتوز في الدم يجب أن تستهلك النظام الغذائي اللاكتوز والجلوكتوز مقيدة خالية
من منتجات الألبان والنباتات موسيلاجينوس. التقييد الغذائي هو العلاج الحالي
الوحيد المتاح لنقص غيل. كما أن البروتين السكري والبروتين السكري الأيض توليد
الجالاكتوز الذاتية، ومع ذلك، لا يمكن حل الجالاكتوز في الدم النوع الثالث فقط من
خلال تقييد الغذائية
======